Lived experience researcher and provider roles require drawing on experience of mental or physical disability to inform research, policy, training service providers and shaping services to better meet the needs of patients. I realised through performing lived experience roles that it is a complex process. The roles challenge the idea of what it typically means to be a patient, that historically is submissive toward the service provider. Through channelling my lived experience into this work, I was able to turn my experiences of mental illness into sources of knowledge that service providers could learn from. I felt like I was making a difference and realised this work had a positive impact on my identity. This led to an interest in wanting to learn more about the influence of these roles on identity and see what research on the area says about this. The image for this blog combines part of an abstract self-portrait with the EMERGES framework, themes found in my research that influence identity. This image brings together personal and professional aspects of myself, common themes found in this work.
A systematic narrative review
As part of my PhD I conducted a systematic review of the literature, alongside a research team, to understand the identity of lived experience researchers and providers. We aimed to develop a framework to explain this in an accessible way. The lived experience researcher and provider term refers to roles such as experts by experience, service user representatives, survivor researchers, service user researchers, peer workers, lived experience practitioners, and mental health professionals with lived experience.
13 studies were included in the review. Identity was understood through roles or social groups people belonged to. We found identity of lived experience researchers and providers typically required navigating both lived experience and professional aspects to the work. Their identity could be understood through professional and service user identities that occurred in conflict with each other (unintegrated), sometimes both professional and service user identities occurred simultaneously (integrated), and sometimes identity was somewhere in between professional and service user (liminal/ambiguous identities), not quite one or the other.
Professional Identity was enhanced through training, qualifications, appropriate job titles, and communicating with other professionals, legitimising the status of lived experience researchers and providers. There were ideas of what it meant to be professional such as not being angry and “having everything together.” (Wilson et al, 2018, p 363).
Service user identity was stigmatised and held less power and status. The experience of being a service user or survivor led to working in these roles. Applying titles like the expert by experience reduced the stigma of being a service user.
Integrated identities meant simultaneously occupying professional and service user identities. This was more difficult to achieve as it required disclosure of lived experience. On occasions their disclosure led to destigmatising disability and demonstrated to colleagues how to integrate lived experiences into their own work.
Unintegrated identities were more common where individuals flitted between professional and service user identities depending on context and who they were talking to. This was influenced by perceived stigma of disability and evaluating whether disclosure was safe or useful. Stigma stopped some from seeking help when relapsing due to perceived expectations of what it means to be a professional, that is viewed as separate to what it means to be a service user.
Liminal identities affected peer researchers and peer workers, where they were perceived as somewhere in between professional and service user. This impacted work relationships and confusion over whether they were colleagues, peers or a different relationship. This “in between” state was hard to navigate, resulting in emotional burden, suggesting a need for additional support.
The EMERGES framework
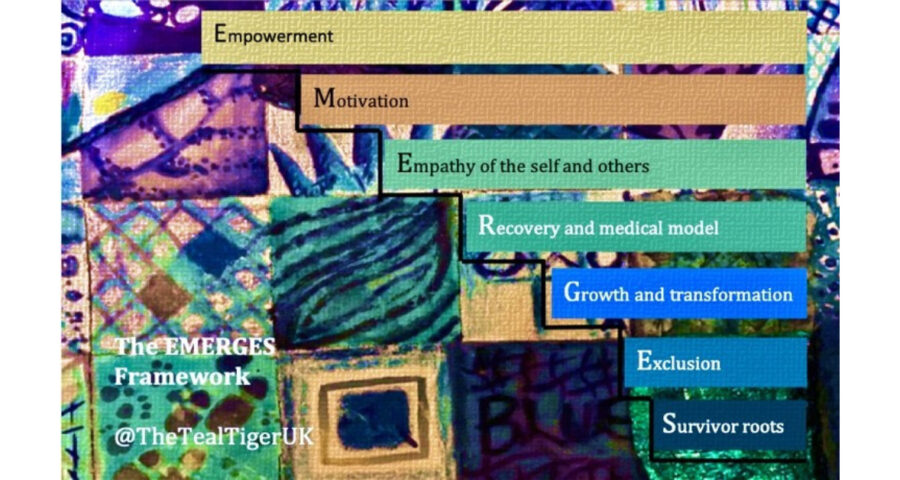
The review found themes related to identity development, through the acronym of the EMERGES framework, a novel finding of the review. Themes of Empowerment, Motivation, Empathy of the self and others, Recovery model and medical model, Growth and Transformation, Exclusion and Survivor roots were found. Moving through the EMERGES framework from survivor roots through to empowerment, were the typical stages in identity development.
Survivor roots was a motivating factor to perform these roles through having survived the mental health system. Both positive and negative experiences of the system fuelled a desire to give back or purposely disrupt the current system and make it fit for purpose.
Exclusion was a theme identifying barriers in this work such as tokenistic involvement. Certain voices that were more articulate were given a platform over others with less professionalised traits. Those from ethnic minorities, carers and those with learning disabilities were often excluded from this type of work.
Growth and transformation came as a consequence of performing these roles and facilitated recovery. “Seeing everybody still ‘fighting for it’… the enthusiasm is more than ever… these are different people to the ones three years ago, I’ve been able to watch my teammates blossom!” (Hutchinson & Lovell, 2013, p 646). Integration of lived experience led to growth of those in these roles, and of the service or research project they worked for.
The recovery model and medical model theme covered the power dynamics in this work. The system often “shifted back to medical model approach” (Cameron et al, 2019, p 1323), recycling ideas of what it means to be a service user, for example, having less power, being ill or disordered. In contrast, the recovery model led to positive identities that were not disordered and hopeful of recovery. Although, ideas of recovery excluded those with chronic disabilities.
Empathy of the self and others came through sharing experiences where they felt heard and understood. They could make sense of their own experiences through listening to others’ experiences. The roles provided a sense of “group survivorship.” (Hill et al, 2021, p 6).
Motivation to integrate their lived experience was important to each lived experience researcher and provider, “It almost comes worthwhile because you can almost see you’re doing something with it.” (Cooke et al, 2015, p 239). This turned lived experiences into sources of knowledge and expertise, making services and research studies more person-centred.
Empowerment came from moving beyond the service user identity through combining existing skills from personal lives with professional skills, leading to greater power and control over their lives, employment prospects and hope for the future.
The EMERGES framework helps me understand my experiences as a lived experience researcher. The stages of the framework can be used as points for reflection for those in these roles and those they work with to identify support needs at each stage in the framework. It can help navigate these roles and support the growth of emerging identities in lived experience work. This is a pre-print of the review.
References
Cameron, Moore, Nutt, et al. (1 more author) (2019) Improving understanding of service-user involvement and identity: collaborative research traversing disability, activism and the academy. Disability & Society, 34 (7-8). pp. 1312-1331. ISSN 0968-7599
Cooke, Daiches, & Hickey (2015). Narratives of experts by experience: the impact of delivering training in partnership on the subject of personality disorder. The Journal of Mental Health Training, Education and Practice, 10(4), 234-244.
Gupta, V., Golding, L., Eames, C., Greenhill, B., Qi, R., Allan, S., Bryant, A., Fisher, P. (2022, June 20). Understanding the identity of lived experience researchers and providers: A conceptual framework and systematic narrative review. https://doi.org/10.31234/osf.io/gjh2c
Hill (2021) Service user and carer representatives’ experiences of the personal effects of involvement in clinical psychology training. DClinPsy thesis, University of Nottingham.
Hutchinson & Lovell (2013). Participatory action research: moving beyond the mental health ‘service user’ identity. Journal of psychiatric and mental health nursing, 20(7), 641–649. https://doi.org/10.1111/jpm.12001
Wilson, Vannice, Hacksel, & Leonard (2018) Peer worker or client?: conflicting identities among peer workers engaged in harm reduction service delivery, Addiction Research & Theory, 26:5, 361 368, DOI: 10.1080/16066359.2017.1410704

My name is Veenu Gupta. I am a lived experience researcher doing many roles that fit under that label. I am an expert by experience for a clinical psychology course, a service user advisor to the National Clinical Audit of Psychosis and EXTEND early intervention care in psychosis study, advisor on the Lancet Psychiatry commission into psychosis, and currently doing my PhD at University of Liverpool. In these roles I draw on my lived experience of mental illness and services to support service providers to better learn from these experiences. In my research I aim to understand the lived experience researcher and provider role and their support needs. I write a blog called The Teal Tiger to make sense of my personal and professional experiences.